

What is the medical industrial complex, and how does it control everything from medical training to patient care? In this first episode of our podcast series, we’ll explore the various ways “ethical medicine” is a misnomer as long as profit is prioritized over healing.
This is the first episode in our series on “Transforming the Medical Industrial Complex.” Our additional episodes can be found here:
Part II – Ableist Constructs of Mental Health
Part III – Transformative Justice and Healing
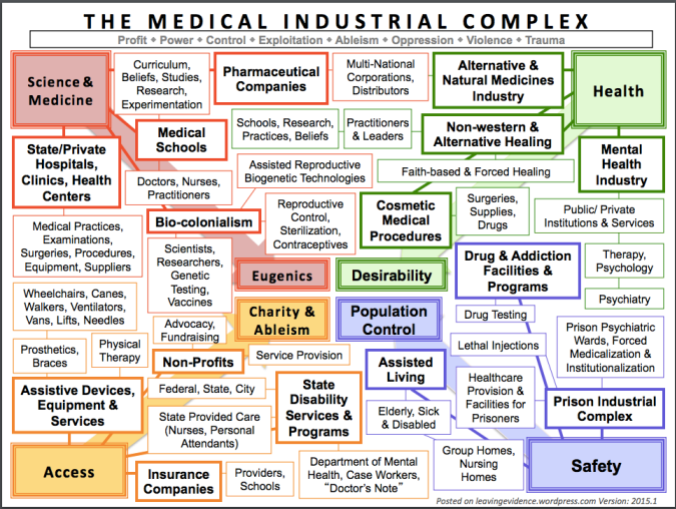
[The image shows a visual layout of the Medical Industrial Complex, which is written at the top in large letters. Just under it, there is a thin, long box that contains the words: Profit, Power, Control, Exploitation, Ableism, Oppression, Violence, Trauma. There are four main quadrants of many different small boxes with text in them, varying in sizes. Each quadrant is in a different color. The boxes are all connected to each other with bolded and thin lines, forming a web-like effect, filling the entire page. There are main categories and subcategories differentiated by bolded text. The boxes are organized according to the outline listed below. In the outer four corners are 4 large boxes with bolded text. The top two on either side read “Science and Medicine” and “Health” and the bottom two on either side read, “Access” and “Safety.” In the middle of all the little boxes, in the middle of the visual are four large boxes that correspond to the 4 outer large boxes. The top two read, “Eugenics” and “Desirability” and the bottom two read, “Charity and Ableism” and “Population Control.” There are 4 large arrows behind the boxes that connect each outer corner large box to its respective middle large box. Science and Medicine is connected to Eugenics; Access is connected to Charity and Ableism; Safety is connected to Population Control; and Health is connected to Desirability. In the bottom right corner there is small grey lettering that reads, “Posted on leavingevidence.wordpress.com Version: 2015.1]
Audio Transcript:
Kelly Park (KP)
Andy Su (AS)
Albert Liu (AL)
KP: Hello everyone! Welcome to the Free Radicals Podcast. Today the topic of our discussion will be on the medical industrial complex [MIC], which is a term that we will revisit in the podcast to explain a little bit better. We will have a series of three episodes that will talk about how medicine interacts with social justice. My name is Kelly, and I’m a member of Free Rads. My pronoun is she. And the reason why I’m really invested in this topic is because I’m a first-year medical student at USC (University of Southern California), where we see a lot of patients at the LA County Hospital, which serves the community around it, which is primarily low-income non-English speaking people who are pretty disenfranchised. It’s a place where you see pretty clearly how things like inequality, structural discrimination, and poverty all impact health outcomes, and how the medical professionals themselves interact with that. I’m here today with two of my good friends, Andy and Albert. Would you like to introduce yourselves?
AS: Hi everyone! My name’s Andy. My pronouns are they/them, he/him. I’m also part of the Free Rads collective, and I was there for the first podcast that we had. I’m here again to provide a social justice framing and probing questions, especially around how the MIC plays into our system of ableism and how it hurts people with disabilities and how it upholds ideals of health and desirability that damage all of us.
AL: Hi everyone, my name is Albert. My preferred gender pronoun is he. I’m here as a guest speaker for Kelly and Andy and the Free Rads podcast. As a fourth year medical student at UCLA, I’m here to provide a perspective since I’ve gone through some [clinical] rotations*. I’m interested in internal medicine, and actually just matched for residency*! Down the line, I’m interested in the intersection between social justice and cardiology, and bringing preventive cardiology into public health.
KP: I hope everyone is excited. I wanted to begin with a vignette that we often see in discussions of medical ethics, which is a pretty common discussion topic at medical school, especially at USC. And this is how it goes: “a homeless patient needs a replacement of his prosthetic heart valve. After his first replacement, he continues to abuse intravenous drugs. Is it a waste of medical resources to replace his heart valve yet again?” How do people feel about that?
AS: I think for me, what is so striking is the framing of the question. So I’m curious as to what is the purpose of the vignette, and what are medical students expected to learn from answering this framing?
AL: Well, I think when we’re posed with that kind of question, the idea is to look at how there is a limited amount of resources and there is this homeless patient who is kind of “to blame” that he has gotten a heart valve and is now using IV drugs. Is there something “wrong” with this situation? Should we [as doctors] spend our “precious medical resources” to replace his heart valve, given that he’s using these drugs again? There’s tension for medical students in how they are supposed to be humanistic and provide care to everyone, but there is this patient in the vignette who is being framed as someone who is to blame and who has habits that are “not good,” and maybe isn’t deserving of our care. If you look at the vignette, it doesn’t really address the systemic issues that create this situation. Why is this homeless patient in this situation in the first place? Why are we not thinking about those issues and addressing those issues, but instead boiling it down to this homeless patient who’s taking IV drugs?
KP: Yes, I agree completely. And to answer Andy’s question about why this question is asked and what we’re supposed to say in response: I think the kosher answer is that we’re supposed to use an ethics algorithm that takes different stakeholders into consideration so that we don’t rely on our gut instinct, which is perceived to be very flawed. What is scary to me is what Albert mentioned — how it fails to take into consideration the deeper moral burden that we all bear in creating this scenario of “ethical uncertainty.” I think the way we talk about it is very flawed, [such as] talking about these things in a one-on-one context between a doctor and a patient, but not talking about why homelessness exists. For example, some reasons some homeless people use drugs are because they need it to stay awake to protect what few possessions they have, or they need it to stay warm at night. And these reasons are not thought about when we think of a stereotypical homeless person, who is an IV drug user, whose situation is “unredeemable.” And that’s why this question is even being asked of us.
AS: I think just the framing of the vignette, as Albert touched upon it: is this person deserving of medical resources? I think that’s such a twisted question, because to him, yes of course, it’s not deemed a waste. It wouldn’t be a fair question to ask him. But this question is posed to medical students or doctors, who have to weigh money and profit over saving a human life or sustaining human life. I think that is so dangerous. It’s such an indicator to the power that doctors have in the medical system over other people.
KP: Right, and the reason why we opened with that vignette is because we wanted to show how there are limits in the way we talk about problems in medical school that go beyond the science and technology of health. And we wanted to use the framework of the medical industrial complex (MIC), which is a topic that’s been discussed by more than one person, but we are primarily operating with the framework laid out by Mia Mingus and her blog leavingevidence.wordpress.com. I highly encourage everyone listening to go check out her blog, especially her post about the MIC, because there is a wonderful visual that captures what we wanted to talk about. For those of you who have not encountered this term before, a basic definition that we generated together is that it’s an oppressive system that focuses on profit rather than the health and wellness of patients. And more dangerously, it’s a system that creates industries that profits off our lack of health rather than contributing to our wellness. I wanted to ask Albert, who is the only one here who interacts with other doctors on a regular basis and is [practically] a doctor himself, do doctors think in this way? Do they talk about what the MIC is and what it does in their lives and what it does to their patients?
AL: That’s an interesting question. When I was preparing for this podcast, I asked around and asked my classmates: do you know what the MIC is? Most of the time I got blank stares. It’s never really talked about in the curriculum. And even as a third or fourth year medical students on the wards, it’s not addressed. I think a lot of time medical students and doctors are just a part of the system, and now that I’ve been doing research on it and seeing it in action, I can see it. But when you go through medical school, you become indoctrinated into everything and don’t really realize what’s going on. And I don’t think, at least at UCLA, there isn’t a lot of talk about the MIC in general.
KP: Yeah, I think that’s pretty unfortunate. Because there are aspects to naming the system and breaking it down that have helped me in thinking about a lot of these issues. In that visual [from Mia Mingus], there are four tenets of medicine and agreed-upon goals by society in how we talk about medicine. Those four tenets are: 1) Science and Medicine, 2) Health, 3) Access, and 4) Safety. These are fairly neutral terms — and possibly even positive terms — that we all would not see as dangerous to ourselves, but what the [visual of the MIC] really lays out is that these four goals are actually motivations for things that are more oppressive. So for example, the goal of Science and Medicine has led to something like eugenics — technologies that erase people, and technologies that place value on certain lives. The goal of Health is used as a motivator for desirability. The goal of Access is used as the motivator for charity and ableism. And Safety is another goal that is used as a motivator or excuse for techniques of population control. I think the homeless patient scenario is a good example of how the last goal of Safety is used instead [of healthcare] to marginalize certain populations. We would only ask that question [in the vignette] because we fear and mistrust homeless people. We [through the MIC] don’t think that they have the ability to take care of themselves. So the flipside to that vignette is that this person is not deserving of that life-saving procedure, and we are actually leaving them to die which helps us eliminate “undesirables” to maintain this illusion of Safety. I think that’s a framework we want to continue talking about as we move through our discussion.
AL: I think another interesting aspect of the homeless patient scenario, building on my experiences at the homeless clinic at UCLA: it’s really striking that homeless clinics are one of the only places where it’s acceptable for medical student care to be the de facto standard of care. When you go into a hospital, medical students are not allowed to treat patients; they’re under the supervision of a doctor. But when you get to homeless clinics, in schools all over the country, even though there is an attending doctor on staff, who’s supposed to be in charge, the expectations are totally different. [Homeless clinics] are popular among first- and second-year medical students because they are a way for inexperienced medical students to get clinical experience. And it’s really problematic in my view, building on what Kelly said about how we see homeless as “dangerous” and “not desirable,” so we kind of as a society permit medical students who are inexperienced to take charge of [homeless people’s] medical care.
AS: That is disgusting! Oh my gosh, I think that plays into the Science and Medicine tenet of the MIC, where science and medicine is a body of knowledge that needs to be taught and practiced. Science and Medicine is a motivator for eugenics, and you see that play out in this scenario. Within eugenics, we will deem homeless people as people who capitalism has failed, but it’s okay, because they can be “subjects” for students to operate on. Oh my gosh, this is so disgusting.
KP: There’s this assumption that they’re not deserving of real medical attention. What was scary to me, when I was first looking at applying for medical schools, is that a lot of medical schools would tout their clinics where they serve homeless patients as a wonderful opportunity for students to further their education, and it was all to provide a needed service. But it always put me off when they bragged about it, because what it was actually saying was that the students who practice on these people, this is going to benefit them more. They would never put these [students] on a wealthier patient, because wealthier patients are more “deserving” of proper medical attention. And the way it was framed to me was just really despicable. While I don’t think USC has too much of an issue with that — I think there is a student clinic, but it’s not too big, it’s sort of folded under the LA County Hospital system where medical students are asked to go in once every week for four hours and we’re assigned a patient who we basically interrogated. Sorry to put it that way, but we basically interrogate them for an hour about all aspects of their health history because we have to practice taking an interview. And we are asked to fumble our way through physical exam where they are asked to remove items of clothing, where we compromise their sense of privacy. As someone who’s had so little practice with that, I feel like it’s so exploitative for us to do that. But all our professors and instructors will say, this is how it’s done. There is no other way for you to learn. And that’s the scary part. That everyone is really invested in this idea that, at all costs, we must train these future doctors. But those costs are pretty heavy to the people who have to bear it.
AL: I think it’s hard too as someone who was the coordinator of one of these homeless mobile clinics. I do see there is a lot of good being done, and we were sort of talking about the systemic issues that lead to homelessness. And there was some effort, in terms of the clinic and the people invested in it, to address some of those systemic issues and work on them. But I do think the biggest problem is how, like Kelly was saying, the way it’s framed that the mobile and homeless clinics are the best thing that these homeless patients are going to get so that they should be grateful. And there’s a lot of good that we’re doing. And it’s true that there is a lot of good being done, but the way that it’s being marketed to medical students as a place where you can come and gain experiences off of these homeless patients is kind of the problem.
AS: I think it speaks to the Charity and Ableism aspect of the MIC. While access to medical care is something we strive for, this becomes charity in the form of these homeless clinics where med students can come in and provide this wealth of knowledge for [these patients] at low to no cost. This speaks to the real problem around access and how healthcare costs a lot, and this concept of using “medical resources” on people is a real indicator of the power and exploitation of the medical industry.
AL: I think if we look at these four loci that Kelly described, one of the aspects that I kind of saw while rotating as a third year medical student was population control. One of my first rotations was on obstetrics and gynecology*. And one of the things I noticed while in the resident clinic, which is the clinic for medical patients and those who don’t have private insurance, is how much of an emphasis there was on contraceptives and birth control. I remember there was a counselor whose sole responsibility was being up to date about the methods of birth control and going around to discuss birth control. At the time, it was framed as beneficial in how we want to make sure that these women, who might have unintended pregnancies, have these methods as a way to empower them. But looking at the way that these birth control methods were counseled towards the women, I distinctly remember a lot of methods were the long-acting birth control methods like the IUDs and Depo-Provera, which lasts 3 months and can have a lot of side effects like bone loss, weight gain. And a lot of these side effects were kind of glazed over and weren’t discussed in detail to these patients. If you think about it in terms of population control, I think that initial framework of empowering these women so that they’re in control of their pregnancy becomes a little more problematic because these are long-term birth control methods that are reversible but it’s not that easy. Then we get into the idea of why are we using these long-term birth control methods, and then we talk about these ideas about compliance and whether or not we think patients can comply with our medical treatment, and I think that brings up a whole other host of issues.
KP: Mhm. And to talk more about reproductive justice, I think that the counseling of certain types of women to use certain types of contraception is the just latest in a line of a really violent and traumatic history of forced sterilization. So for example, in the 1960s and 70s, a bunch of poor Latina mothers at LA County Hospital were sterilized against their will, or were sterilized in a way where they had no choice but to sign the papers because the nurses would withhold needed medication or anesthesia until they signed that paper. I highly recommend a documentary called No Más Bebés, a documentary by Renee Tajima-Peña. It’s an account of these women who endured that history and who tried unsuccessfully to sue the hospital and the doctors that did this to them. And it’s scary to me because the doctors who were interviewed in that documentary kept talking about how they really believed that what they were doing was good, that they did not think that they were forcing these women to something that was harmful to them, and that at that point, I think nationally a lot of doctors truly believed that it was better for certain women not to reproduce because it would create a burden on society. And now it’s manifested as aggressive birth control counseling, and it’s talked about — like Albert said — in an empowering way, but I don’t think we should forget about its really racist and traumatic history.
AS: I think Albert you had brought up in previous conversations about that difference of how birth control is suggested for low-income women vs in wealthier hospitals or private hospitals?
AL: I rotated at the resident clinics and more in the private clinics, and I think the way that difference manifested was when the obstetricians and gynecologists were talking about options with the women who had private insurance, it was much more of an equal conversation where the woman was advocating for her health and the provider was giving a bunch of options, really discussing what were the pros and cons of each medication. It was very much a talk among equals, whereas at the resident clinic I felt like it was very much pushed upon, like we think this is good for, we want this for you, and so there is a difference in power dynamics.
AS: And that speaks I think to power and control that is allowed in the MIC that leads to the violence and the trauma. I think this speaks more to the Access and Ableism and Charity piece because I think I want to explore how the MIC helps uphold ableism and perpetuates that system of violence. So for those who aren’t familiar, ableism is loosely defined as a system and a set of practices and beliefs like other -isms, like racism and sexism. In this case ableism is a set of practices and beliefs that assigns an inferior value or worth to people who have disabilities — say for example, developmental, emotional, physical and psychiatric disabilities — and holds them of a lesser value and privilege than people who are able-bodied, or people who don’t have these disabilities. I think access is a big piece to it because ableism manifests in that oppression through the lack of power that people with disabilities have. The MIC directly profits off of it by providing very necessary health care for people with disabilities that they need to survive, but this care, this service, is seen as a charity. It’s seen as “oh you don’t have access to this, but we’ll provide it for you. We have the power to do that.” And when you have this dynamic of power it leads to control, it leads to exploitation, and it leads to violence and trauma. For example, a very simple way that this plays out in the power that doctors have over people who might know their [own] health care and their health needs more is the doctor’s note. For example, if you needed to get out of class or if you needed some kind of validation of pain and a health problem that you’re going through, you need a verification from an official doctor in the form of a doctor’s note. And that’s the only way that it can validate something that you’re going through, even though you know that yourself, “oh I’m not feeling well,” or “oh, this is hurting me.” But you can’t validate that unless you have the power of a doctor behind you. And I think that’s so scary!
AL: I think that also kind of manifests not only in how people have to interact with the system but also how doctors view their patients. I think that kind of power is kind of internalized when students become doctors. When I’m in the hospitals during rotations, I see [who doctors call] typical “WebMD” patients who look up their symptoms and come into the doctor’s office and hospital with a lot of questions about their symptoms and what they mean, and challenge and question the doctor and try to advocate for their own bodies. I think a lot of doctors tend to think of those patients as “difficult” because they’re not really processing what their doctor’s saying and taking it as the truth and accepting it blindly. And so you have the “difficult” patient who is trying to challenge the doctor, but also the easy patients who just accept everything the doctor is saying and I think that ties into the MIC nicely because the issue is that difficult patients take more time, and when you have to spend a lot of time counseling patients and convincing them to take a medication or to follow through with a treatment plan, that’s time not spent with another patient, time not spent billing and generating more revenue codes.
AS: I think that hinges on the profit aspect of the MIC because it would make more sense for doctors to sit down and counsel through a patient and really work through so that they understand what they’re prescribing or what the problem was so the long term preventive care can happen. But that takes time, and time is money, and money is something that doctors don’t actually have a lot of or don’t have the luxury of being able to provide really the high-quality care they want to provide. So [it’s a] contradiction where doctors would want to provide or it would make sense to provide this high quality care for a long-term preventive measure but they’re not able to because of the MIC.
AL: Yeah, and I’ve seen a lot of medical students who come into medical school being very idealist about wanting to help patients and believing in preventive care and counseling patients, [but] when you get caught up in rotations and being busy all the time and the sheer volume of patients you have to see, it just becomes very difficult to keep that perspective. I know a lot of my classmates who want to counsel patients and want to spend that time but just can’t because of pressures. And it’s a very sad thing to see.
KP: I think that also begs the question why people in general don’t know more about their health. I think part of the reason why people turn to stuff like WebMD is because we really — and I’m speaking as someone who is not a doctor — we really don’t have information about our own bodies and about health and nutrition. It is unbelievable to me that we are not taught these things as soon we enter school. I feel like it’s so important for our existence and our wellness — much more important I think than taking calculus or physics… I mean these things are important for knowledge, general knowledge but they’re not going to define how you survive in the world, on a very basic, fundamental level of existence. And it occurs to me that in the framework of the MIC, which prioritizes profit over everything, it really benefits that system for people to be denied that knowledge and that wisdom about their own bodies because as long as that knowledge is kept within the gates of academia and within just the brains of doctors who have to go through years and years of training, that gatekeeping enables us to profit off of that highly rarified knowledge. It’s still something that I cannot wrap my mind around, why we spend so much time in [K-12] school learning things that I never use now but I’m only learning important things about my body because I have made the big decision to go into medical school.
AL: That’s interesting. I think that ties in also to our view of patients in private hospitals vs public county hospitals. I kind of touched upon this earlier with the idea of the “difficult” patient but I think when I ask my classmates, “why do you like working with patients in the county hospitals, these lower-income, poorer patients, people of color?” A lot of the responses are, “I feel like these people are grateful, these people listen to what I say.” On the surface that’s great, it’s nice to have grateful patients as a doctor; you feel like your work is being validated, but there’s something about that in terms of what Kelly was saying, the gatekeeping of knowledge. The fact is that a lot of these patients don’t have a lot of health literacy and so they’re not really able to challenge what the doctor is saying and really advocate for their own bodies, and the fact that we as medical students and doctors are taught to appreciate that means that there’s something with the medical system, and the fact that we don’t appreciate when patients engage with us and challenge us, that doesn’t seem right.
AS: Yeah, and again I’ve spoken at length about how this system of profit and denying people access to care, denying people access to knowledge, allows for power and control which leads to ableism and exploitation, oppression, violence, and trauma. And this power where people cannot challenge doctors, they cannot challenge larger systems for the sake of their own health and well-being, and that can lead to a lot of violence where doctors can abuse their power, and abuse the trust of patients. This takes place for example in the forced sterilization of the Mexican immigrant women. It happens also in the MIC where there are patients who have been sexually assaulted, sexually abused, and are not in a position to challenge that because of the doctor’s power, and the doctor’s assumed knowledge and years of training.
KP: I think that’s a really great example of how the MIC ends up controlling people who don’t have as much power in society. I think another way that doctors maintain that power is that I think we [doctors] define what wellness means, we define what able-bodiedness means, and that enables us to profit off of it, because we not only get to ask the questions, but we also have all the answers. We are the only ones in power to give them those answers. And it’s this really neat, closed loop that shuts out all other perspectives.
So this is really tough question for me to ask, but I will ask it anyway: what is it that we as medical students, as future doctors can do within this system? How can we make it better for our patients and for society? How do we start dismantling the MIC?
AL: Well I think the first step honestly is just becoming more cognizant of the forces that are at play in the medical system. The way we introduced this topic was when I was talking about how a lot of medical students don’t really understand or even know about all these topics that we’ve been discussing, and just being aware of them and how it affects your interactions with your patients. I think that the smallest focus of change is our actions with our individual patients, and just treating all patients with the respect, and not feeling that tinge of annoyance when someone is trying to understand their care, trying to understand your diagnosis and your treatment because like you were saying, Kelly, it is a closed loop. You make the diagnosis and you prescribe the treatment and when the patient is trying to engage with you and feel a little more empowered, take the time as a provider to engage with them. Maybe not teach them but just kind of explain to them your reasoning and let them feel more in control. I think that kind of one-on-one interaction can spread to your entire patient panel and slowly the culture of medicine.
AS: And building on that interpersonal is really important and going beyond and recognizing the system the MIC plays out and how Kelly said, it’s a closed loop, it’s a system that starts with the diagnosis from doctors who gatekeep the knowledge to the pharmacy or the medicine providers that then profit off of your deemed lack of health. So challenging that system, we bring in other ways of understanding, other forms of knowledge. One form of sociological study is recognizing disability studies. One of the pieces on our Free Radicals blog written by Alexis, one of our own good founders, about how she was trying to develop a cure for her neurodivergent brother through neuroscience but recognizing all the while what he really needed was a community of care, a community that respected his neurodivergence and didn’t exactly label as mentally ill, as something that needs to be restored. Understanding how the MIC creates these bodies of knowledge, creates this concept of health and wellness that is profitable and challenging that and recognizing that as you’re in your studies, [think about] how “does what I’m learning and participating in actually put profit over people?” When what all people need sometimes is a recognition of their humanity and being allowed to exist in a way that might be deemed “unhealthy,” but recognizing that the label [of unhealthy] is just for the sake of profit and not for the sake of their well-being.
AL: Yeah I think that a lot of times when we as doctors have defined diagnoses and treatments and when a patient doesn’t really fit in with the diagnosis or we have trouble identifying what is exactly is wrong and we don’t have a clear cut treatment for it, that patient can end up becoming ostracized because they keep coming in for treatment and the doctor doesn’t really know what’s wrong with them. That’s kind of seen as a failure, as someone who can’t be profited from, and so when that patient comes in for the 10th visit, there’s always this sigh of disgust. As a provider, recognizing that that happens and just not allowing yourself to feel those emotions and to respect that patient and what they’re coming with and recognizing that while you might not be able to treat them, they are still deserving of your kindness and humanity is one small step you can take.
KP: I absolutely agree that education and awareness within the medical community is really important. But I also would like to advocate for general education starting at a younger age within our schools so that people are more empowered to understand how their bodies work and to be an advocate for themselves, and to take away power from the medical establishment. And I say this as someone who will have a lot of power. I don’t think it’s good for me and I don’t think it’s good for anyone.
I wanted to put in a plug for our next two episodes where we will explore a little bit more about the things we were talking about. Our next one will be on how the MIC hurts patients — we’ll be looking at it with a more close lens. We talked a little bit more today on the bigger picture, but we really want to look at the details of how it’s affected people. Our third episode will explore how we can change the MIC from within and how we can move toward a model of transformative justice and community accountability rather than just individual interventions. And finally, I wanted to put in one last request that people read Mia Mingus’s website, leavingevidence.wordpress.com. Without that blog and without that breakdown of the MIC, none of us would be sitting here having this discussion. Thank you for listening, and we hope that you continue listening to our future episodes.





